- Anesthesiology Malpractice
- Posts
- The Death of Joan Rivers
The Death of Joan Rivers
Case #29
I remember hearing about this case when it occurred, but the details were unclear.
I had read what was published in the lay press, but they rarely get it right.
After reading through the court documents, it was even worse than I thought.
The anesthesiologist handwrote a 4-page document which will be referenced throughout. Some of it may be difficult to read on mobile, so I have transcribed it.
An 81-year-old famous actress presented to a GI center for an upper endoscopy.
She had a history of chronic GERD on long term PPI medicine, voice hoarseness, and high blood pressure.
A 20g PIV was inserted into her forearm and she was brought to the endoscopy room.
Dr. B (anesthesiologist) wrote the following note about Dr. C (GI) and Dr. K (ENT).

“Dr. C introduced Dr. K as an ENT surgeon. I noticed she had scrubs on. Timeout was performed at 09:04am. Then, the patient, Dr. K, and Dr. C had a discussion regarding her case. At 09:09am patient removed her dentures and gave them to her physician and then moved into the left lateral decubitus position. Dr. C placed a bite block in her mouth while I gave 100mg propofol for sedation via a 10cc syringe. Patients vitals stable. Dr. C then requested Dr. K to perform her procedure which I wasn’t aware of until that moment.”


Become a better anesthesiologist by reviewing malpractice cases.
Free, paid, and CME options available.
This ENT (Dr. K) has a practice that caters to celebrities and singers.
She is a “voice specialist” and only takes cash.
Joan Rivers followed with her for voice hoarseness.
Dr. K had brought a small portable nasal endoscope (it was not a video scope and only Dr. K could see through the eye piece).
After ignoring the anesthesiologist and performing flexible nasal endoscopy, she could not get an adequate view of the larynx.
She withdrew her scope.
The EGD begins:

“At this time patient started to move, so I gave an additional 20mg propofol. During EGD patient vitals stable with O2 flow at 2L/min. Upon insertion of gastroscope, the area immediately surrounding the vocal cords was found very edematous and there were thick mucoid secretions which were suctioned by Dr. C with the EGD scope.


“I expressed my concern about the airway edema and the possibility of airway compromise with future manipulation with Dr. C. I further requested Dr. C to insert his EGD scope so I could visualize what was being done during laryngoscopy. Dr. C said it was not necessary and that I was being paranoid. Then he proceeded to take pictures of the surgeon and patient with his cell phone.”
The ENT performs her procedure again

“At ~9:28am during the second laryngoscopy, patients O2 sat started dropping below 95%. I started jaw thrust, asked tech to increase O2 flow to 6L/min and asked Dr. K to remove her scope. Despite this, patient’s O2 sat kept declining below 90%. I asked the tech to give me an oral airway and ambubag ready on the cart already connected to O2 outlet. So at 9:29am I started ambu bagging with 100% O2 at 15L/min with an oral airway in place and a tight seal. It was difficult ambubagging her at first as I was giving forced breaths to get air in her and some chest rise with breath suggesting possible laryngospasm in addition to already noted airway edema.”
The anesthesiologist asked for another pulse ox to check if a low reading is real.
The GI commented he could not feel a pulse and the HR was noted to be 40bpm.
ACLS was started and help called. Atropine, epinephrine, lidocaine were administered.
2 other anesthesiologists arrive to help.

“Dr. (Anesthesiologist #2) attempted an oral intubation but was unsuccessful and then I attempted to look with a MAC 4 laryngoscope but could not identify landmarks due to severe edema and could not visualize the patients vocal cords. I then asked Dr. (Anesthesiologist #2) that we need to get the emergency trach/cric kit and video laryngoscope ready and looked for Dr. K, the ENT surgeon for possible tracheostomy. She could not be found in the procedure room. I then attempted to intubate her and was successful with a MAC 4 blade and deep cricoid pressure only able to see the tip of vocal cords. I use a 6.0 ETT. Intubation was difficult due to severe edema, poor visualization, and a very anterior larynx.”
Soon after intubation, paramedics arrived and the patient was transferred to the hospital.
She did not wake up and had imaging consistent with global anoxia.
Joan Rivers died 1 week later.
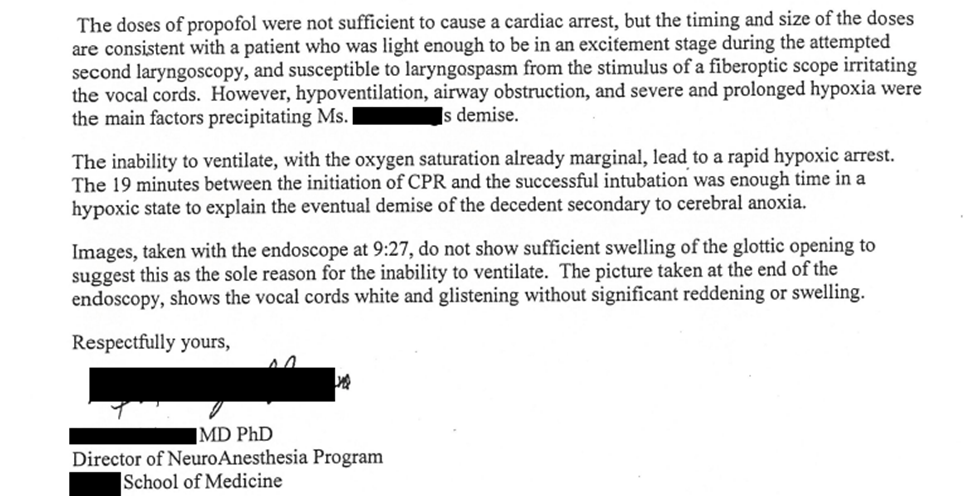
A neuro anesthesiologist at the hospital gave his opinion to the medical examiner.
The GI doc claimed he had no such cell phone pictures from that day.

Outcome
The settlement was confidential.
The endoscopy center lost its accreditation with CMS and with the American Association for Accreditation of Ambulatory Surgery Facilities, which affects reimbursement.
NYS DOH investigated the clinic and found a variety of safety lapses.
The GI doc stepped down as medical director.
Learn to defend yourself from malpractice cases.
Whether each lawsuit is frivolous or warranted, there’s always something to learn.
MedMalReviewer/Anesthesiologist Analysis
I created a short summary of the lapses in the case:
No one was aware this ENT would be there
There was no signed consent for this procedure
The ENT did not have privileges at this endoscopy center
The anesthesiologist’s pre op concerns were ignored
The anesthesiologist’s concerns over the second ENT look were ignored
The GI doc took cell phone pictures of the anesthetized patient with the ENT
The ENT abandoned the patient when she was decompensating and may need a trach
There was an element of VIP syndrome that led to all these safety lapses. It is unclear if the patient requested her ENT be there to perform this procedure, or if this was volunteered to her as a favor. Either way I am willing to bet Drs. K and C would not arrange this for a non-celebrity. I had a mentor who would say special patients who get special treatment get special results. This article from Cleveland Clinic is worth a glance; Nine Principles for Caring for VIPs. Principle number one is to not bend the rules.
I was curious if there was any disciplinary action taken against the ENT Dr. K. Both the Office of Professional Medical Conduct (OPMC) and the quality improvement organization for Medicare (Livanta) conducted separate investigations. Directly on Dr. K’s website she advertises these investigations found no wrongdoing on her behalf for the death of Joan Rivers. I could not find any evidence of disciplinary action against the anesthesiologist or GI doc.
Joan Rivers had one daughter who inherited most of her estate. She was quoted as saying the settlement allows her to “put the legal aspects of my mother’s death behind me and ensure that those culpable for her death have accepted responsibility for their actions quickly and without equivocation.” Her estate was worth an estimated $150 million, so it’s fair to say this one really wasn’t about money. There was obvious fault and no point in prolonging the process or dragging anything through a trial. A settlement makes sense here.
In case anyone skimmed the neuroanesthesiologist’s letter, he hypothesized the ENT scope irritated the vocal cords during the procedure which directly caused the laryngospasm. This was more than just propofol, secretions, and an unlucky laryngospasm, but once again the direct action of the ENT. In this case we saw a plastic surgeon receive criminal charges and jail time for performing a procedure inappropriately. I think all the involved physicians here are very lucky a settlement is all that came from this.
Reply